 HEALTH
HEALTH
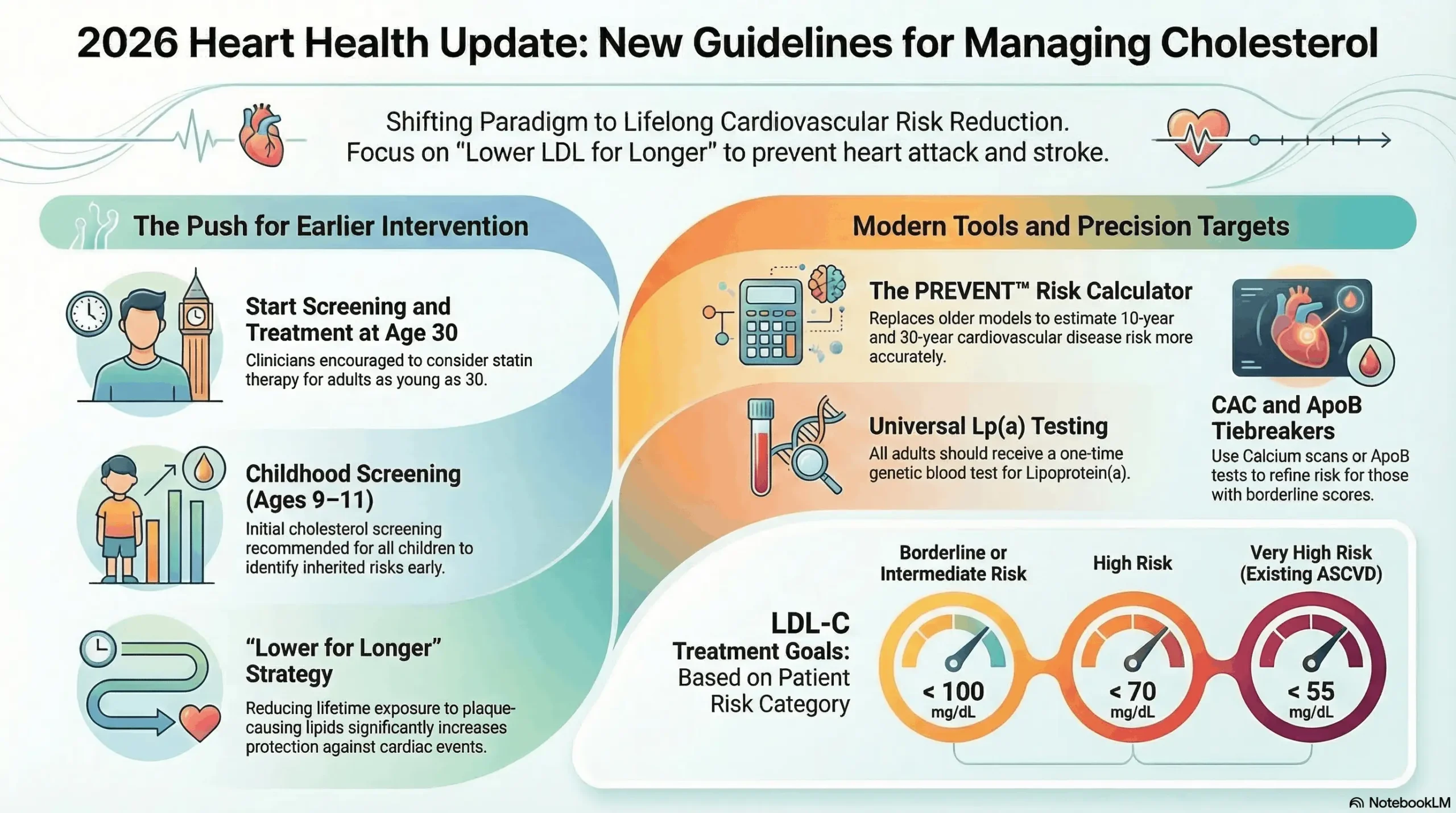
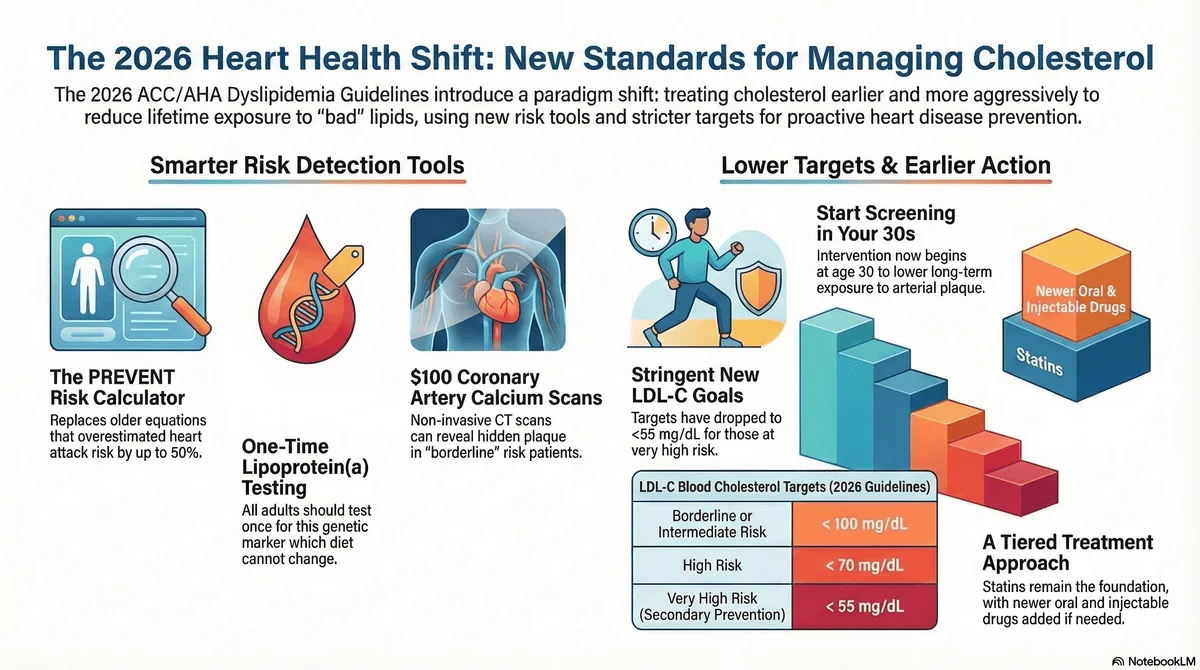
Washington/Dallas — The American College of Cardiology and the American Heart Association have released updated clinical guidelines for the management…
March 17, 2026
•
5 min read
 HEALTH
HEALTH
Washington/Dallas — The American College of Cardiology and the American Heart Association have issued updated clinical guidelines for managing abnormal…
March 15, 2026
•
4 min read
 HEALTH
HEALTH
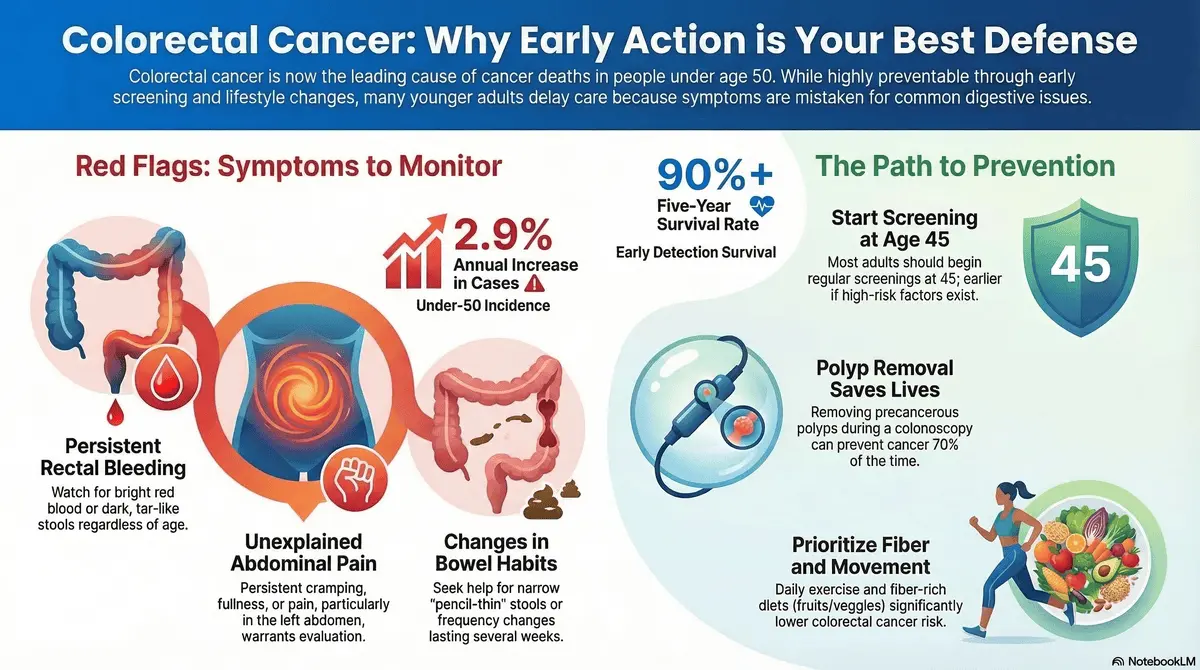
Washington/New York — Colorectal cancer has officially become the leading cause of cancer-related deaths among adults under the age of…
March 13, 2026
•
5 min read
 HEALTH
HEALTH
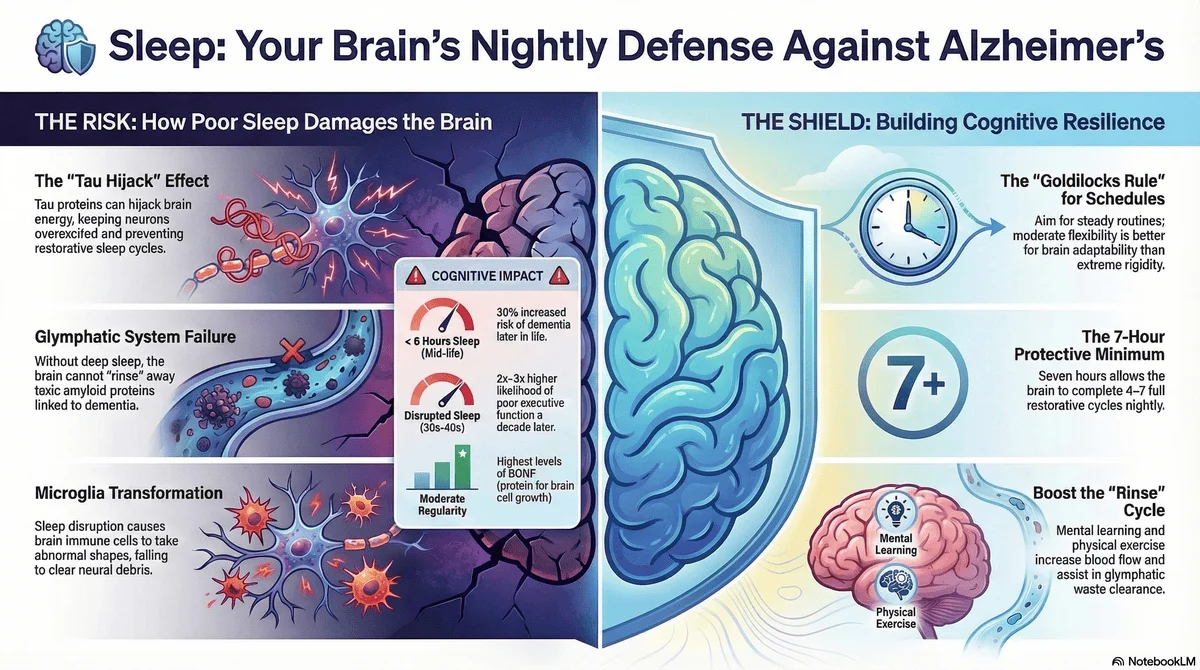
Lexington/College Station — Recent scientific investigations have revealed how irregular sleep patterns directly contribute to neurodegenerative conditions like Alzheimer’s disease.…
March 12, 2026
•
6 min read
 HEALTH
HEALTH
Atlanta/New York — Medical professionals nationwide are raising alarms over the increasing incidence of colorectal cancer among younger demographics, a…
March 11, 2026
•
5 min read
 HEALTH
HEALTH
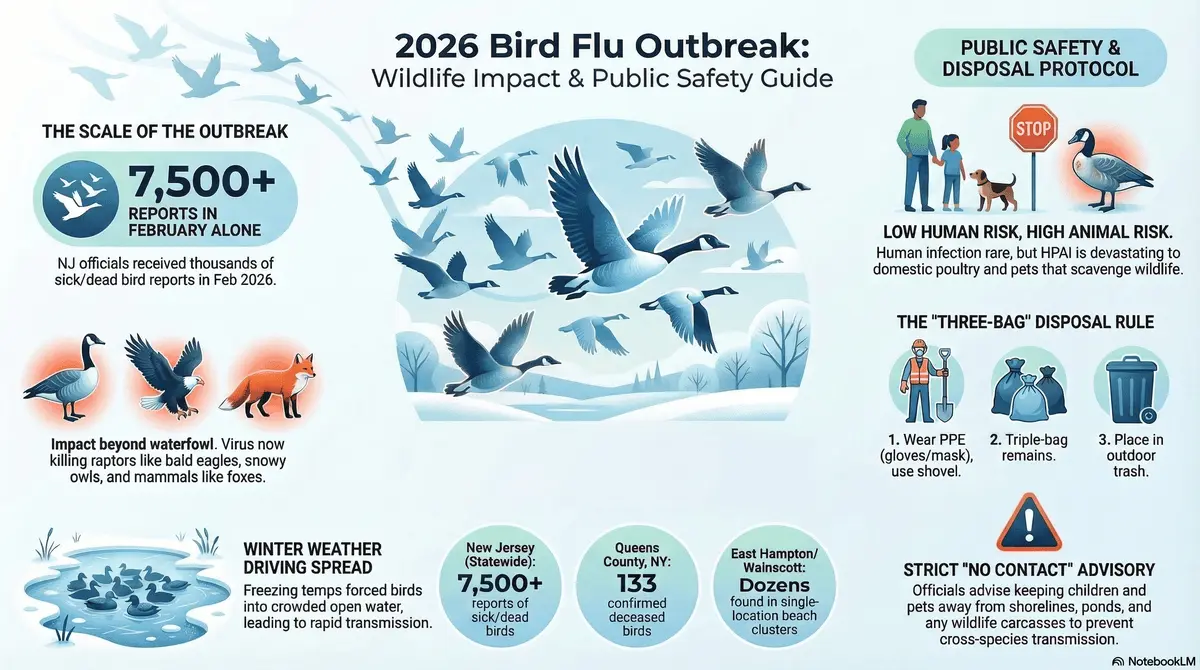
New York/New Jersey — Health and environmental agencies are monitoring a rapidly expanding mass mortality event affecting wild birds, predominantly…
March 9, 2026
•
6 min read
 HEALTH
HEALTH
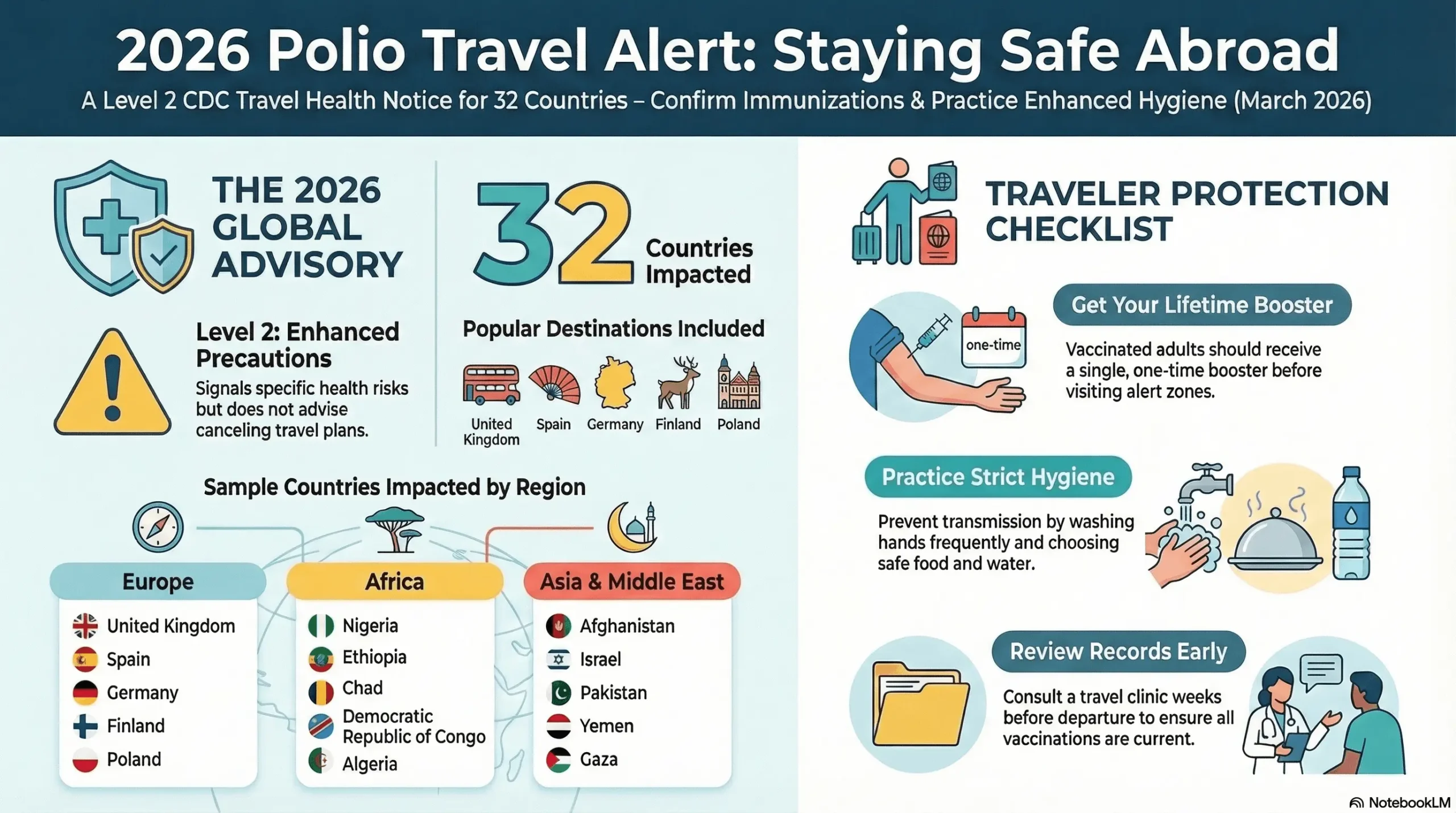
Atlanta — The U.S. Centers for Disease Control and Prevention has issued a Level 2 global travel health notice urging…
March 7, 2026
•
5 min read
 HEALTH
HEALTH
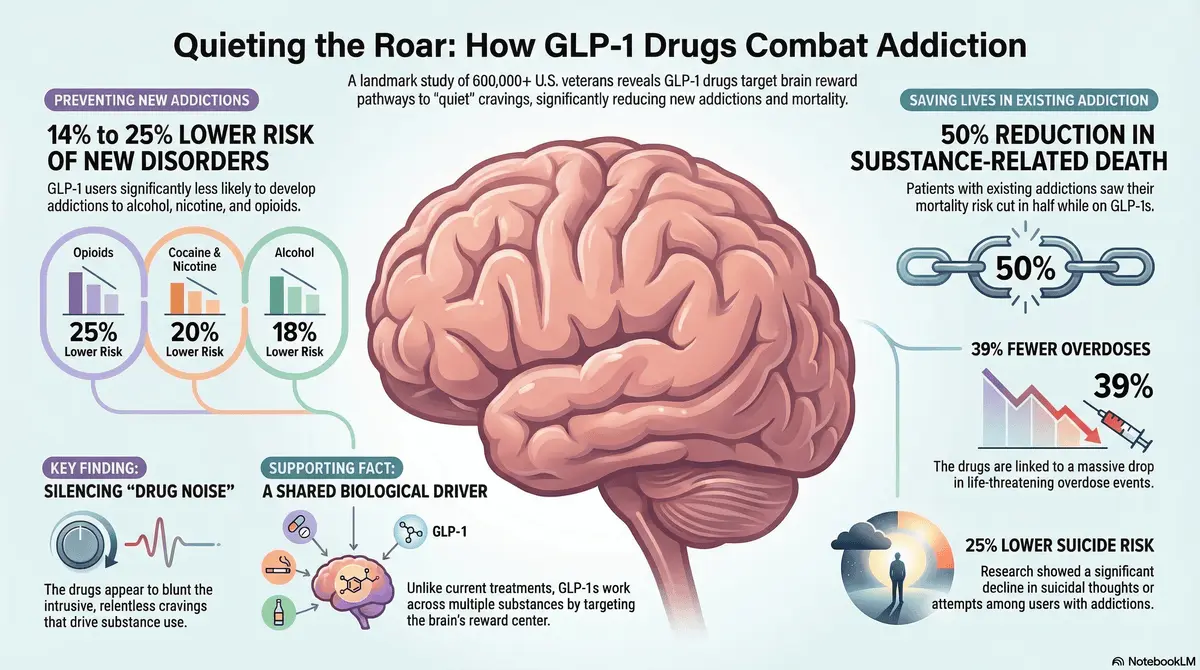
St. Louis—A comprehensive new study has revealed that GLP-1 receptor agonists, blockbuster drugs widely known for treating diabetes and obesity,…
March 5, 2026
•
5 min read
 HEALTH
HEALTH
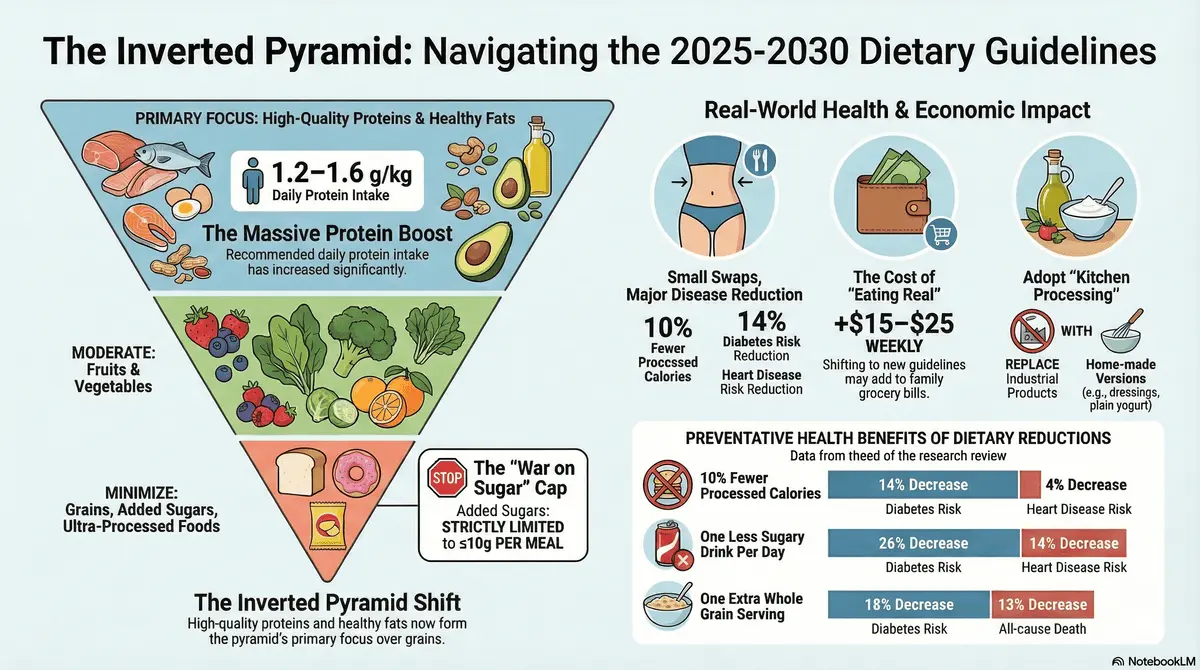
Washington, D.C. — The United States government has released the 2025-2030 Dietary Guidelines for Americans, fundamentally altering federal nutritional advice…
March 1, 2026
•
5 min read
 HEALTH
HEALTH
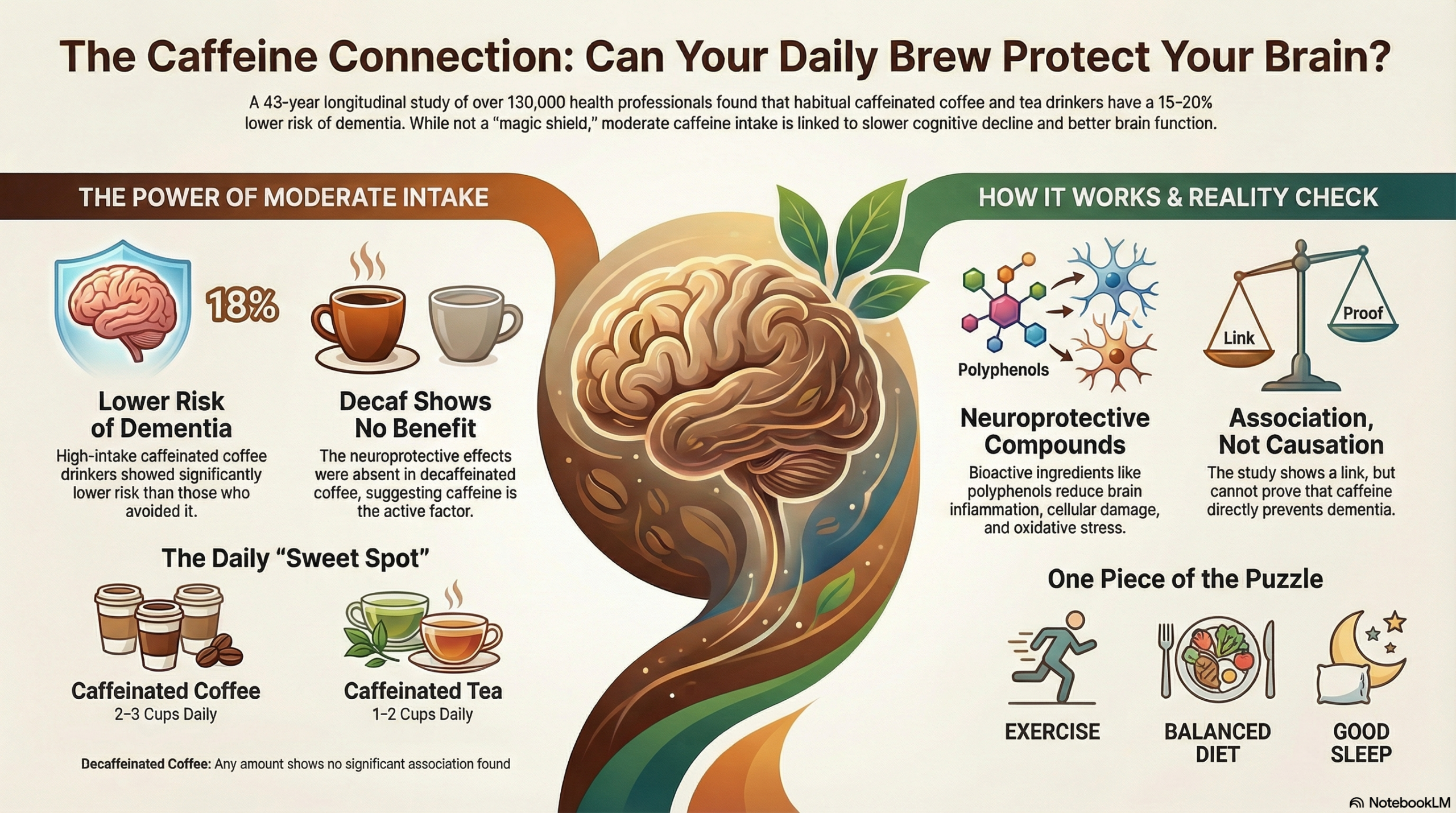
Boston, Massachusetts — A landmark long-term study published in the Journal of the American Medical Association (JAMA) in February 2026…
February 12, 2026
•
5 min read