Washington/Dallas — The American College of Cardiology and the American Heart Association have released updated clinical guidelines for the management of dyslipidemia, lowering the age for intervention and introducing a new cardiovascular risk calculator. The comprehensive update, published on March 13, 2026, replaces the 2018 guidelines and focuses on long-term lifetime cardiovascular risk reduction. By encouraging earlier screening and more aggressive lipid-lowering therapies, the organizations aim to significantly reduce the risk of heart attacks and strokes.
Below is a detailed breakdown of the new cholesterol guidelines and their impact on patient care.
Context & Background
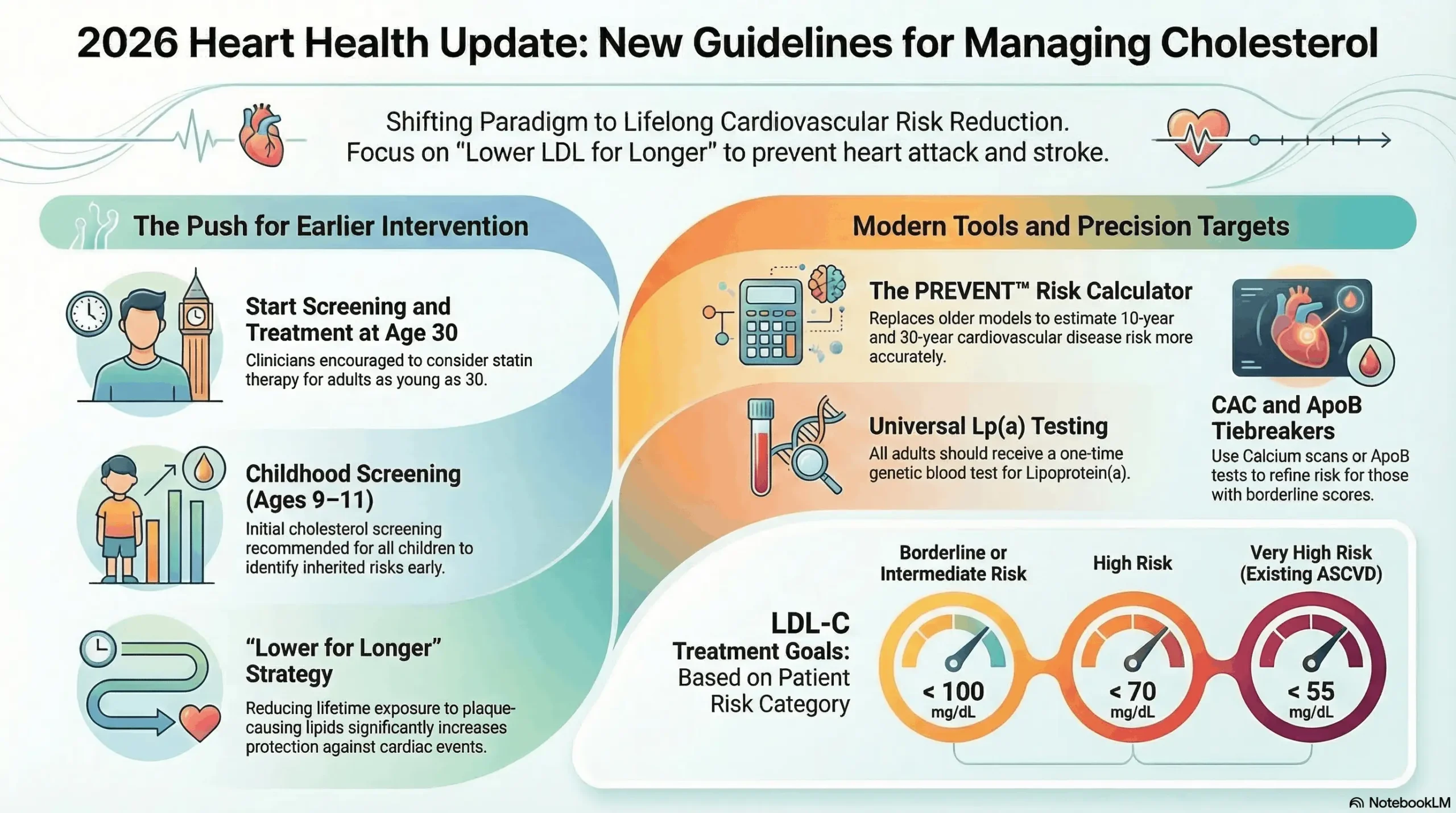
The Shift to Lifetime Risk Assessment The updated guidelines represent a paradigm shift from assessing just the 10-year risk of cardiovascular events to incorporating 30-year risk projections. Clinicians are now directed to use the PREVENT-ASCVD equations, which replace the older Pooled Cohort Equations that often overestimated risk. This modern calculator allows for a more personalized evaluation of atherosclerotic cardiovascular disease (ASCVD) risk in younger populations, prompting earlier intervention.
New Biomarker Recommendations A major addition to the framework is the recommendation to perform universal, one-time screening for Lipoprotein(a) during adulthood. Because Lp(a) levels are primarily genetically determined, this test helps identify families with high inherited risk for cardiovascular disease without the need for repeat testing. Furthermore, the guidelines suggest measuring Apolipoprotein B (ApoB) and utilizing coronary artery calcium (CAC) scans to refine risk assessments in borderline or intermediate cases.
Reestablished Treatment Goals Unlike previous iterations, the 2026 guidelines bring back specific target levels for low-density lipoprotein cholesterol (LDL-C). Medical professionals are urged to help patients achieve an LDL-C level of less than 100 mg/dL for those at borderline risk, less than 70 mg/dL for those at high risk, and less than 55 mg/dL for individuals who have already experienced a secondary cardiac event.
The Focus on Youth and Prevention Recognizing that high cholesterol begins to impact heart health early in life, the guidelines stress the importance of screening children between the ages of 9 and 11. If lifestyle modifications fail to control lipid levels, healthcare providers, such as Dr. Roger S. Blumenthal and Dr. Pamela B. Morris, encourage initiating statin therapy much earlier, potentially for adults in their 30s.
Q&A: Unpacking the 2026 Dyslipidemia Guidelines
Q: How do the PREVENT-ASCVD equations change the way doctors assess cardiovascular risk?
A: The new PREVENT model provides a more accurate, long-term projection of an individual’s likelihood of developing atherosclerotic cardiovascular disease by evaluating both 10- and 30-year risks.
- Age Expansion: The calculator evaluates adults aged 30 to 79, encompassing younger demographics previously overlooked by short-term risk metrics.
- Risk Categorization: Patients are classified into low (<3%), borderline (3% to <5%), intermediate (5% to <10%), and high (10% or higher) 10-year risk brackets.
- Personalized Enhancers: The tool factors in unique risk enhancers such as chronic kidney disease, HIV, inflammatory conditions, and high-risk ancestry.
Q: Why is early intervention via statin therapy heavily prioritized in the 2026 update?
A: Medical experts determined that prolonged exposure to high LDL cholesterol significantly increases lifetime cardiovascular risk, making early suppression crucial.
- Plaque Accumulation: Reducing lipids earlier in life minimizes the long-term accumulation of plaque in the arteries, which causes heart attacks and strokes.
- Dosage Benefits: Starting treatment in a patient’s 30s may allow for lower doses of statins, thereby reducing the likelihood of side effects like muscle pain or liver damage.
- Secondary Options: If statins are insufficient, the guidelines endorse combining them with nonstatin therapies like ezetimibe, bempedoic acid, or PCSK9 inhibitors.
Q: How does the new guideline approach the screening and management of Lipoprotein(a)?
A: The guidelines elevate Lp(a) testing to a Class 1 recommendation, mandating it at least once in adulthood to capture hidden genetic risks.
- Genetic Stability: Because Lp(a) levels remain relatively stable throughout a person’s life and are largely unaffected by lifestyle changes, a single test is deemed sufficient.
- Cascade Screening: Identifying high Lp(a) in one patient allows doctors to screen siblings and children, catching severe familial hypercholesterolemia earlier.
- Risk Thresholds: An Lp(a) level of 125 nmol/L (50 mg/dL) correlates with a 1.4-fold increased risk of a cardiac event, while 250 nmol/L doubles the risk.
Q: Why are coronary artery calcium (CAC) scans recommended for certain patient demographics?
A: CAC scans are utilized to detect early, subclinical plaque buildup to help resolve uncertainty regarding whether a patient should start lipid-lowering medication.
- Target Demographics: Non-contrast CAC scans are advised for men over 40 and women over 45 who fall into borderline or intermediate risk categories.
- Treatment Thresholds: The presence of any amount of coronary calcium supports adjusting the patient’s LDL-C goal to below 100 mg/dL.
- Plaque Visualization: By physically measuring the calcified plaque in artery walls, doctors can offer a more concrete assessment than statistical equations alone.
Q: How do the guidelines address high cholesterol in children and adolescents?
A: The guidelines introduce pediatric screening recommendations to establish a baseline and intervene before long-term arterial damage occurs.
- Screening Window: Universal cholesterol screening is recommended for all children between the ages of 9 and 11.
- Lifestyle Foundation: Early detection allows families to implement dietary changes and exercise routines to naturally manage lipid levels.
- Pharmacotherapy Consideration: For youth with familial hypercholesterolemia, doctors may consider introducing medication early to prevent severe adult-onset disease.
Editorial Note & Transparency
Verification Log:
- Medical Organization Reports: Sourced directly from press releases and guidelines from the American College of Cardiology and American Heart Association.
- Medical Journals: Findings cross-referenced with publications in Circulation and the Journal of the American College of Cardiology.
- Expert Testimony: Incorporates direct statements from guideline writing committee members like Dr. Roger S. Blumenthal and Dr. Pamela B. Morris.
Compliance:
- Privacy: This article respects user data under our Privacy Policy.
- Transparency: No sponsored content influenced this reporting.
Contact Us: For corrections or feedback, please email: news.desk@qnanews.com