Washington/Dallas — The American College of Cardiology and the American Heart Association have issued updated clinical guidelines for managing abnormal blood lipids to prevent cardiovascular disease. These guidelines were jointly published in major medical journals on March 13, 2026. The new framework recommends earlier screening starting at age 30 and utilizes a novel risk calculator to assess long-term cardiovascular threats.
Below is a detailed examination of the updated guidelines and their clinical implications.
Context & Background
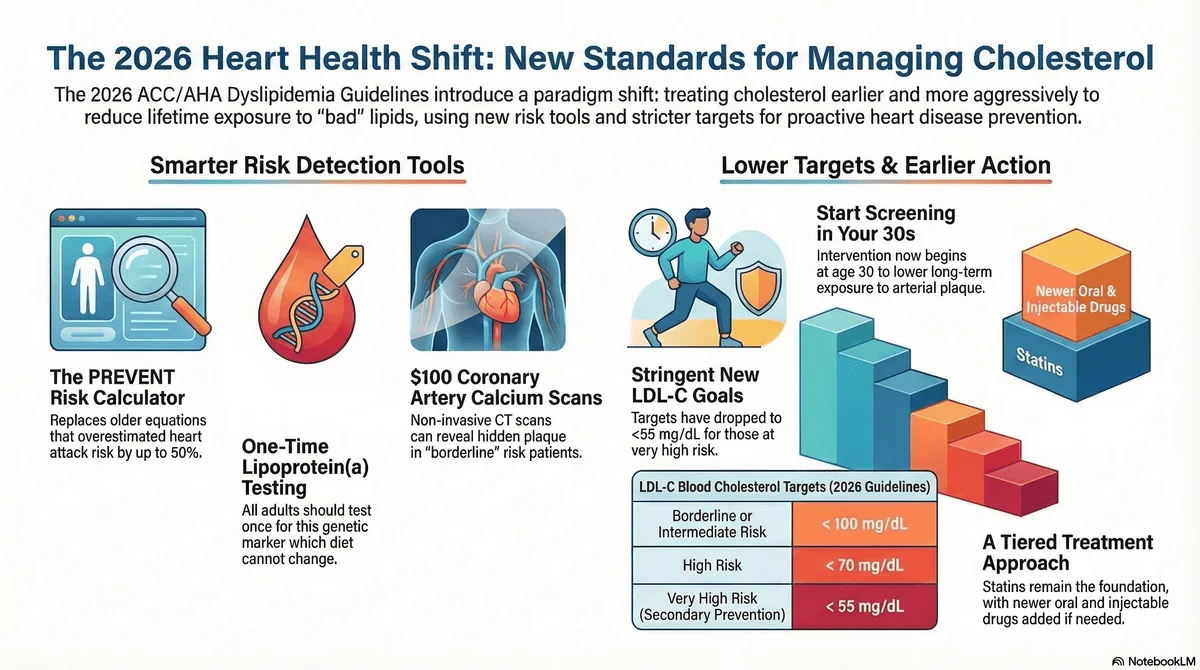
Why did the guidelines change? The update addresses the reality that earlier risk calculators overestimated 10-year risk and failed to capture the lifetime exposure danger of atherosclerotic cardiovascular disease (ASCVD). Experts determined that lowering low-density lipoprotein cholesterol (LDL-C) earlier in life provides significantly greater protection against future heart attacks and strokes.
The Key Players The new framework was developed collaboratively by the American College of Cardiology and the American Heart Association, alongside nine other prominent medical organizations. Significant contributors include Roger S. Blumenthal, chair of the guideline writing committee, and Pamela B. Morris, the committee’s vice-chair.
Shifts in Clinical Targets The guidelines reintroduce specific LDL-C and non-HDL-C targets, urging doctors to treat borderline or intermediate-risk patients to under 100 mg/dL and very high-risk patients to under 55 mg/dL. While statins remain the primary pharmacological tool, earlier initiation is encouraged alongside foundational healthy lifestyle changes like diet and exercise.
Q&A: Unpacking the 2026 Dyslipidemia Guidelines
Q: How does the new PREVENT calculator alter cardiovascular risk assessment?
A: The PREVENT calculator replaces older models to provide both 10-year and 30-year risk estimates for patients starting at age 30.
- Target Demographics: It evaluates adults ages 30 to 79 without known ASCVD or subclinical atherosclerosis.
- Risk Tiers: It classifies 10-year risk into low, borderline, intermediate, and high categories to guide lipid-lowering therapy.
- Personalized Enhancers: It incorporates risk enhancers like family history, chronic kidney disease, higher-risk ancestry, and reproductive risk markers to refine scores.
Q: Why is lipoprotein(a) testing now recommended for all adults?
A: A one-time test for lipoprotein(a) is advised because elevated levels are an inherited, stable marker of significantly increased cardiovascular risk.
- Genetic Stability: Levels are largely genetically determined and minimally affected by lifestyle changes, making repeat testing unnecessary.
- Risk Escalation: A level of 125 nmol/L or greater correlates with a 1.4-fold increased long-term risk of a heart attack or stroke.
- Clinical Decision-Making: High levels can help doctors determine whether a patient requires aggressive lipid-lowering medication earlier in life.
Q: How do the new guidelines approach the use of non-statin therapies?
A: The guidelines endorse a tiered approach of non-statin therapies for patients who cannot achieve their LDL targets through statins and lifestyle changes alone.
- First-Line Alternatives: Ezetimibe and bempedoic acid are recommended as primary evidence-based oral add-on options.
- Injectable Options: PCSK9 monoclonal antibodies are supported for patients requiring more intensive LDL-C reduction.
- Clinical Validation: At this time, the long-term clinical outcome efficacy of inclisiran remains unverified by official sources and is still undergoing clinical trials.
Q: Why is coronary artery calcium (CAC) scoring utilized under the new framework?
A: CAC scoring is used selectively as a non-invasive imaging tool to detect early plaque buildup and refine treatment decisions for uncertain cases.
- Scoring Demographics: It is recommended for men over 40 and women over 45 who fall into borderline or intermediate 10-year risk categories.
- Treatment Adjustments: The presence of any calcified plaque supports aiming for an LDL-C goal of less than 100 mg/dL.
- Target Refinement: Higher amounts of detected calcium warrant even lower, more aggressive LDL-C target levels.
Q: How does the framework address cholesterol management in pediatric populations?
A: The guidelines emphasize early detection by recommending universal cholesterol screening for children to mitigate lifetime ASCVD risks.
- Screening Window: Screening is advised for all children between the ages of 9 and 11 who have not been previously evaluated.
- Inherited Risk Identification: Early screening helps detect inherited lipid disorders and other lifestyle-induced elevations.
- Intervention Strategy: Collaborative care involving clinicians, parents, and caregivers focuses on proactive lifestyle adjustments before adulthood.
Editorial Note & Transparency
Verification Log:
- Medical Journals: The Journal of the American College of Cardiology and Circulation.
- Official Statements: Press releases and statements from the American Heart Association and the American College of Cardiology.
- Expert Commentary: Clinical insights from lead cardiologists including Roger S. Blumenthal, Pamela B. Morris, and Steven Nissen.
Compliance:
- Privacy: This article respects user data under our Privacy Policy.
- Transparency: No sponsored content influenced this reporting.
Contact Us: For corrections or feedback, please email: news.desk@qnanews.com